
Click on image for active links:


Information about DCIS can be overwhelming. Here is a quick reference guide to keep it simple.
Please click image to access the Guide with clickable links.

It’s my 15 year Overdiagnosis Day!
January 19, 2010 — my life changed forever.
This was the day I was given a diagnosis of something I had never heard of before.
It was called Ductal Carcinoma in Situ (DCIS) and it was described as a “pre-cancer.”
But…..because of uncertainty about a potential future real INVASIVE cancer, I was told the treatments were agggressive, the same as if it were invasive cancer.
I was given scary risk statistics, and sent home with an outdated inappropriate booklet called “A Woman’s Guide to Breast Cancer Diagnosis and Treatments.”
I KNEW in my gut something wasn’t right.
This was the beginning of a 15 year investigation that continues to this day!
Every day my heart breaks for women who unknowingly become another statistic of this epidemic.
My websites DCIS 411 and DCIS Redefined provide information which is vastly different from other websites discussing DCIS. These sites not only help women understand the controversy and issues about DCIS overdiagnosis and overtreatment, they also focus on newer safer technologies for monitoring breast health, as well as holistic ways to reduce cancer risk while increasing body, mind, spirit wellness.
Online groups affiliated with my websites have grown from a few women to thousands in the last few years. Women are actively seeking “alternative” information, and those finding my websites and support groups are extremely grateful.
My goal now is to reach more women BEFORE they are taken down the overdiagnosis and overtreatment rabbit hole.
I am working on two ebooks:
1.) “DCIS: The Holistic Way
2.) “MAMOPOLY: What You Need to Know Before You Roll the Pink Dice”
I want to thank everyone who has supported me along the way. Words of kindness, encouragement, and appreciation remain in my heart and motivate me to keep going.
I am equally grateful for all the many naysayers and fear-mongers over the years! I would have never been so fired up to investigate as deep as I have! Thank you for challenging me!
As I strive to improve how I communicate and empathize with all people of different mindsets, I welcome all comments and criticism.
In peace, love, gratitude, wisdom, and health,
Donna Pinto
January 19, 2025
I think we can all agree, when it comes to our health, we would prefer clear information on risks and benefits vs being oversold.

But, when it comes to mammograms, most women do not even realize they have NOT been given informed consent. Many say they feel encouraged, pressured, and even coerced into scheduling a screening mammogram. There is often no mention of risks or harms. Not from doctors, not from breast cancer charities, not from celebrities, and not from the media.
Unfortunately credible resources and good scientific information have been drowned out with marketing slogans.
“Get Your Mammogram! Early Detection Saves Lives.” These messages are heard over and over, but is this doing more harm than good?

This blog post aims to provide women with actual facts and clear information which help provide informed consent to women about mammography screening.
The short definition: “Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a given procedure or intervention. (See longer definition below).
Another issue which overshadows informed consent are all the arguments about various guidelines. When to start, when to stop, how often, and now there is emphasis on newer technology such as 3D or contrast enhanced mammograms. There is even some discussion about dense breast tissue. But women are often still unclear on what to do if they have dense breast tissue.
Examples of Clear Information, Not Marketing
The Harding Center for Risk Literacy created “fact boxes” to illustrate benefits and harms of early detection of breast cancer by mammography screening.
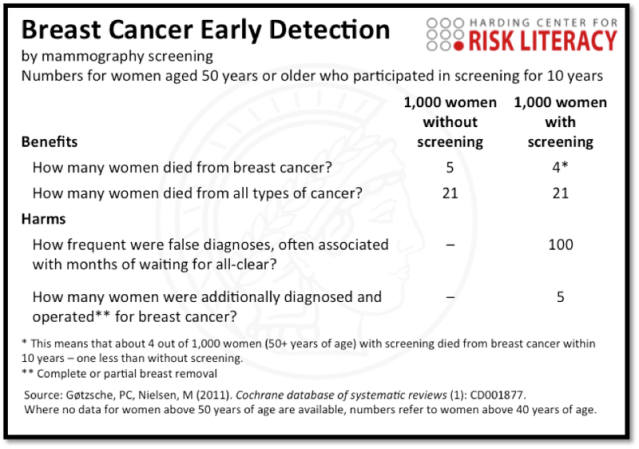

Summary: One life saved out of 1,000 women screened, but 5 lives harmed.
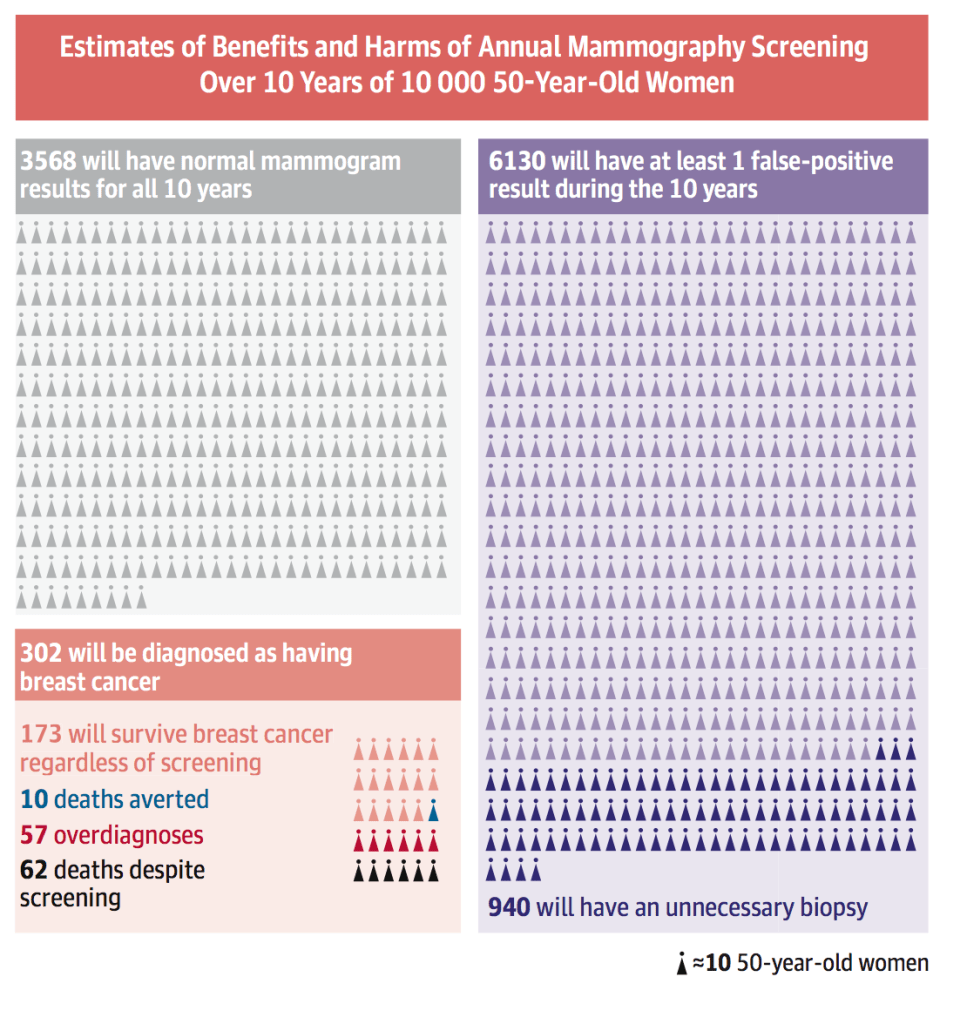
Another chart shows estimates of benefits and harms of annual mammography screening over 10 years of 10,000 women in their 50s:
How many women are having discussions with their doctors about potential overdiagnosis of DCIS and a high chance of having an unnecessary biopsy?
Thankfully science writer Christie Aschwanden studied the issue and has written several articles on the topic in an effort to help women make informed choices. Her article, It’s Ok to Opt Out of Mammograms, is a must read!
Key points from article:
“The premise of screening is that it can find cancers destined to metastasize when they’re at an early stage so that they can be treated before they turn deadly. If this were the case, then finding and treating cancers at an early stage should reduce the rate at which cancers present at a later, metastatic stage. Unfortunately, that’s not what’s happened.”
Screening mammography has failed to reduce the incidence of metastatic disease and it’s created an epidemic of DCIS.
“…widespread mammography, able to detect smaller and smaller lesions, has led to a sevenfold increase in the number of new cases of DCIS. Today it accounts for about one in five breast cancer diagnoses, with some 64,000 women diagnosed with the condition last year.“
Mammography also leads to the treatment of cancers that never threatened the patient’s life, and these treatments can increase mortality.
Did you know –-Mammograms miss 40% of INVASIVE CANCER?!?!
This, too is controversial and a bit taboo to discuss, but it is a very real concern for many women. Doctors often dismiss any harm with statements like, “The amount of radiation is equivalent to flying across the US.”
There is a support group of over 250 women called Victims of Mammogram United.
Medical physicist John Gofman “argued forcefully that radiation is overused in medicine, both for diagnosis and treatment, without a full consideration of the risks.” Gofman and his colleague stated, “the risk from low doses of radiation was 20 times higher than stated by the government.” – LA TIMES 2007
He claimed, “There is NO safe dose of ionizing radiation.” More info here and here.
See chart here about radiation-induced breast cancers from mammography
More recent research about “Mammography-induced cancers” by Daniel Corcos is discussed in video here:
A study published in the prestigious New England Journal of Medicine stated:
Results: …”we estimated that breast cancer was overdiagnosed (i.e., tumors were detected on screening that would never have led to clinical symptoms) in 1.3 million U.S. women in the past 30 years. We estimated that in 2008, breast cancer was overdiagnosed in more than 70,000 women; this accounted for 31% of all breast cancers diagnosed.
Conclusions: Despite substantial increases in the number of cases of early-stage breast cancer detected, screening mammography has only marginally reduced the rate at which women present with advanced cancer. Although it is not certain which women have been affected, the imbalance suggests that there is substantial overdiagnosis, accounting for nearly a third of all newly diagnosed breast cancers, and that screening is having, at best, only a small effect on the rate of death from breast cancer. – Effect of three decades of screening mammography on breast-cancer incidence
Since 2012, I read and collected numerous articles and I wrote several blog posts. After many years, I created a page dedicated to this topic. Overdiagnosis 411
On a mammogram, a silent, indolent tumor looks the same as a deadly, progressive cancer that just hasn’t yet spread. If a clinician finds cancer on a mammogram, it often still triggers a slew of follow-up treatments possibly including biopsies, surgery, chemotherapy, and radiation — all unneeded and harmful interventions if the cancer was destined to remain silent.” – How often is breast cancer overdiagnosed? New research finds true cases far outweigh false alarms
Cancer Research UK states: Overdiagnosis: when finding cancer can do more harm than good
Overdiagnosis, in turn, leads to overtreatment, which is the treatment of clinically insignificant disease, essentially giving too much treatment without benefit to the patient. Treating a cancer that is not life-threatening leads to significant harm for women. Accepting the Swiss Medical Board estimates, that means one in five women who was told she had breast cancer after her mammogram received unnecessary treatment for cancer. The result is that tens of thousands of women in the U.S. each year are treated unnecessarily for breast cancer and undergo surgery, radiation and chemotherapy for tumors that are not and never would be life threatening. – How Routine Mammography Screening Leads to Overdiagnosis & Overtreatment, Breast Cancer Action
1.6 million breast biopsies are performed each year in the US, and approximately 80% are found to be benign.
One study found that false-positive mammograms and breast cancer over-diagnosis account for $4 billion dollars in spending every year.

ABC Investigates featured my story and the problem of overdiagnosis: Is Stage Zero breast cancer really cancer? 7 ON YOUR SIDE investigates the controversy

Women may hear…
“Regular mammograms reduce breast cancer deaths by 20%.”
Sounds pretty good…but how many lives do they really save?
Only 1 in 1,000!
A short video explains in a simple way:
Please read:

Informed consent about mammography screening is important!
“Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a given procedure or intervention. The patient must be competent to make a voluntary decision about whether to undergo the procedure or intervention. Informed consent is both an ethical and legal obligation of medical practitioners in the US and originates from the patient’s right to direct what happens to their body. Implicit in providing informed consent is an assessment of the patient’s understanding, rendering an actual recommendation, and documentation of the process. The Joint Commission requires documentation of all the elements of informed consent “in a form, progress notes or elsewhere in the record.” The following are the required elements for documentation of the informed consent discussion: (1) the nature of the procedure, (2) the risks and benefits and the procedure, (3) reasonable alternatives, (4) risks and benefits of alternatives, and (5) assessment of the patient’s understanding of elements 1 through 4.
It is the obligation of the provider to make it clear that the patient is participating in the decision-making process and avoid making the patient feel forced to agree to with the provider. The provider must make a recommendation and provide their reasoning for said recommendation.” – Informed Consent, https://www.ncbi.nlm.nih.gov/books/NBK430827/
INFORMED CHOICE in Breast Cancer Screening / Insurance for Ultrasound and QT Imaging
A wealth of information to understand all the potential harms of mammography can be found at:

After a day of hiking to Machu Picchu in Peru, I received a text from a friend with a screenshot of a familiar face — Dr. Laura Esserman, Director of the Breast Care Center at UCSF. She was being interviewed on the news. The headline read ELLE MACPHERSON REVEALS CANCER BATTLE.
My friend texted: “DCIS and they are calling it breast cancer and that she is in remission. That she chose to not do treatment. Crazy with being barely cancer… of course you know.“
Eager to connect to Wifi at my hotel that evening, I was shocked by the media blitz criticizing Elle.
One article titled: Elle Macpherson slammed for ‘holistic’ cancer approach stated:
Macpherson’s approach to treatment has been met with criticism on social media, particularly firing up users on X, formerly known as Twitter.
Cancer researcher Dr David Robert Grimes said: “Incredibly irresponsible from Elle Macpherson: Holistic therapy is NOT (a) valid treatment for breast cancer.”
Meanwhile, Dr Liz O’Riordan said: “We have proof that … who choose not to have mainstream cancer treatments for breast cancer are 6x (sic) more likely to die thanks to @sky__john and co.
Another article stated: Doctors from the UK to Australia and back have slammed her pronouncements, with one professor of public health from Trinity College Dublin saying “this bullshit kills people“.

I found myself in disbelief.
DCIS is not life-threatening.
Once I returned home, I was able to investigate further. Thankfully I found one article that actually mentions the incongruency of information and what was missing from the many media articles and comments:
“But media coverage of Macpherson’s situation has largely missed a key piece of information: her breast cancer is not invasive. This missing information from the media is also a missed opportunity to discuss less invasive options for the management of DCIS. The rate of DCIS has increased greatly since the introduction of breast cancer screening. You can detect it on a mammogram but it rarely causes symptoms. Many of these lesions are unlikely to ever cause a problem in a woman’s lifetime. As a result of this, some cases of DCIS are considered to be over-diagnosed. Now options such as active surveillance (closely monitoring but not providing treatment unless the condition progresses) are considered reasonable and are being robustly evaluated in research trials to help reduce overtreatment.”
Since 2009, there have been conferences and debates and published articles calling for the removal of the word “carcinoma” as well as less aggressive treatment options including “active surveillance.” See Medscape article Take Carcinoma Out and Ease off Treatment.
This one article sparked my personal quest of endless hours drilling into the debate among medical professionals. I started to collect articles and videos of the few experts stating DCIS is more like “abnormal cells” and the word “carcinoma” should be removed from the diagnosis because it creates exaggerated fear and too many women felt rushed towards aggressive “cancer” treatments.
DCIS 411 was created in 2011 to educate women about this.
After 15 years of my own personal research regarding DCIS and Holistic Health, seven years serving as a Patient Advocate within high level medical research to help reduce DCIS overdiagnosis and overtreatment, and 13 years hosting a DCIS website and online support groups, I believe my opinions and my questions matter.
Why is the media not helping women to better understand DCIS — that it is not “breast cancer,” but a risk factor?
Why are holistic therapies not being studied to help reduce risk of invasive cancer after a DCIS diagnosis?
I was told by one doctor, “There’s no money in it.”
Elle did what I believe all women should do… slow down, get 2nd opinons, make well-informed decisions, and make your health a priority.
Over the years the media has praised other celebrities diagnosed with DCIS who are champions for prophylactic double mastectomies. In 2015, celebrity chef Sandra Lee spoke out publicly and said her doctor told her she was a “ticking time bomb” which drove her to choose a double mastectomy for DCIS. I wrote DCIS is NOT a “Ticking Time Bomb” — What Women Really Need to Know. I also wrote about the high rate of double mastectemies for DCIS here.
We are all unique and there is no one right way to handle or treat a scary diagnosis like DCIS. I fully relate with Elle’s choices. Although I am not a celebrity with endless financial resources, I too sought multiple opinions from conventional cancer doctors, integrative doctors, naturopathic doctors, a nutritionist, a holistc dentist, and I also sought out and paid out of pocket for different forms of breast imaging. I read nonstop. I studied anti-cancer nutrition. I came to believe wholeheartedly in “Food and Lifestyle as Medicine.”
Now, when I think back to when I received a DCIS diagnosis in 2010, I remember how the aggressive “standard of care” treatments presented to me shocked me more than the actual “pre-cancerous condition” the nurse told me I had. I felt frozen by the thought of losing my breast or having daily radiation for weeks. The anti-hormonal drugs seemed awful, and I was more worried about short and long-term side effects than a slight risk reduction. I knew, from extensive research that if I declined any or all treatments that my life was not in danger.
And it turns out I was right.
Being told “Your breast is like spoiled soup and not worth saving” is truly horrendous. In 2023 I wrote about how I proved my doctor wrong: In 2011, My Doctor Told Me: “Your Breast is Like Spoiled Soup… It’s Not Worth Saving.”
It continues to amaze me that 15 years after this all began for me, the media is still over-sensationalizing a dangerous “cancer battle” of a celebrity who is diagnosed with a non-invasive, non-life-threatening condition.
Not only do I feel the media is doing a disservice to women, I feel doctors have a responsibility to educate the public and correct the media when a celebrity like Elle’s diagnosis is being wrongly discussed and over-sensationalized.
Great to see follow up articles such as this: Elle Macpherson defends holistic cancer treatment despite backlash:
“I guess I would say I’m really pleased that it [has] sparked conversation and discussion, because with discussion comes awareness and comes growth,” she said of the backlash the initial interview had generated. “Uncomfortable for me, but I think it’s very worthwhile in that sense,” she said.
Bravo Elle Macpherson! Let’s keep the conversation and education going!
Please watch my DCIS story on Inside Edition and then click the links below:
Over-diagnosis 411: Overdiagnosis Devastates Lives of Healthy Women
Be W I S E (Screening 411) Women Informed Supported Empowered

I just found out Dr. Michael Lagios, a true legend in the field of #DCIS pathology/research, passed away on April 7, 2024.
While I did not agree with everything Dr. Lagios told me when I consulted with him in Nov 2011, it was evident to me he had a sincere desire to help women make better informed decisions and potentially spare them from a mastectomy and or radiation and tamoxifen. He was a true pioneer at the time and he was the co-creator of the Van Nuys Prognostic Index (VNPI) which classified DCIS into different risk categories and served as an aid to the complex treatment decision-making process.
In my case, despite being given a high risk score (8) on the VNPI, I felt emboldened by Dr. Lagios reviewing my pathology slides and downgrading the DCIS cells to LOW grade. In 2010-2011, there were no women online saying NO to surgery, radiation and tamoxifen/AI and I was being heavily pressured by multiple doctors to have a mastectomy and/or more surgery + weeks of radiation and tamoxifen, despite his new determination that my case was downgraded to LOW grade DCIS.
In my effort to help women gain more insights about DCIS, I asked Dr. Lagios if I could post the recording of my 45 min phone consultation with him. He kindly said yes.
In November 2011, at the time of the consultation, I was still new to a lot of the DCIS research and I was asking a lot of questions. My questions then are still some of the same questions being asked by women newly diagnosed with DCIS today.
One of the most important things I learned, and I feel women who have had biopsies or surgeries with positive margins, will feel peace of mind from starts at minute 27:47. Dr Lagios states:
“Clearly as DCIS, it doesn’t have any metastatic ability. Even if you chop it up surgically and leave it in the wound, it will not become invasive. The cells don’t spill out of the cut-through duct, for example, and then start growing in the breast. It requires several mutations of the cancer cell itself before it develops the ability to invade the breast.“
A few weeks later, I took Dr. Lagios’ advice and drove 1.5 hours for a consult with Dr. Mel Silverstein in Irvine, CA. He suggested a reduction (removing the close margin of DCIS) and lift of both breasts (for symmetry).
Next I flew to San Francisco to have a consult with Dr. Laura Esserman in February 2012. She suggested tamoxifen alone for breast cancer prevention.
The reason I was seeking all these opinions was because my doctor in San Diego had told me:
“You’re breast is like spoiled soup. It’s not worth saving.”
My gut instinct was, No way. I would not even consider mastectomy.
Then she said:
“Don’t be stupid Donna — at least do 3 weeks of radiation.”
She also told me, “You don’t want to wait until it’s not treatable.”
After extensive research into #overdiagnosis, I began to research alternative breast imaging and I found Dr. Kevin Kelly who invented Sonocine automated ultrasound.
Despite Dr. Lagios and many experts saying there was more DCIS in my breast and all of them said, “I wouldn’t do NOTHING…”
I declined all of the treatments.
I never had another mammogram.
I never had another breast issue. (13 years later)
While I defied Dr. Lagios by doing NOTHING (conventional) further, I am forever grateful to him and I hold him in the highest regard.
Thank you Dr. Michael Lagios — for all that you did for me — and for the many thousands of women who came before and after me — seeking to better understand DCIS. May your spirit and wisdom continue to watch over and guide women and physicians alike.
For anyone interested in this topic, please listen to my phone consultation with Dr. Michael Lagios and then spend time reviewing my blog and the HOLISTIC HEALTH path I chose to focus on.

(Photo taken in Kauai, Aug 2023 by Glenn Pinto)
And she was guided by the light
Cut loose like a deuce, another runner in the night
Guided by the light
She got down, but she stayed forever in the light
Yes she’s surely made it all right.
-Adapted from Blinded by the Light, Bruce Springsteen
In 2010, my friend Adriana showed me the light. She set me free from the terror that doctors had instilled in me. I am forever in gratitude. Sharing my story, insights, and resources is my way of paying it forward.
One of my first blog posts was written in January 2012, two years after a DCIS diagnosis rocked my world: You can read it here:

In October 2015, I hosted “Beyond Breast Cancer Awareness,” an event to educate women about options for early detection and cancer prevention.
I made a video for the event to highlight the choice I made to go against medical advice and say NO to overly aggressive “standard of care” treatments.
The video features books, films, videos and more inspiration for creating my websites, support groups, and a nonprofit organization (now called Give Wellness):
A recent update to my story can be found here:
May you, too, be guided by the light.
With love and gratitude,
Donna Pinto, April 2024

An official Presidential Proclamation declaring April 2024 as the inaugural National Cancer Prevention and Early Detection Month states:
“Healthy life habits — like maintaining a healthy body weight and reducing exposure to tobacco smoke — can prevent certain cancers, so we are working to help all Americans get and stay healthy. Our National Strategy on Hunger, Nutrition, and Health supports expanding incentives to purchase fruits and vegetables with SNAP, ensures more kids have access to free and nutritious school lunches, and expands access to nutrition and obesity counseling.”
RIGHT ON!!!
Unfortunately the part about early detection and cancer screenings as a way to “beat cancer” sounds like a great idea, but…
Mammography screening comes with serious harms often not not disclosed to women, thus depriving them of informed consent and informed choice.
Women deserve INFORMED CHOICE in Breast Cancer Screening!
A petition for this is outlined below:
INFORMED CHOICE in Breast Cancer Screening / Insurance for Ultrasound and QT Imaging
Women deserve INFORMED CHOICE in Breast Cancer Screening.
Currently women are told they MUST have a mammogram in order to have an ultrasound.
There are well documented valid concerns about mammography screening.
Many women have already experienced serious harms. Many prefer to OPT OUT of mammography for the following reasons:
– Over-diagnosis of non-invasive “pre-cancers” leads to aggressive overtreatment for tens of thousands of women every year.
– Under-diagnosis (mammograms miss 40% of INVASIVE cancer in dense breast tissue).
– Unnecessary biopsies (80% are “false positives”) may cause pain and injury to sensitive breast tissue.
– Compression and radiation can cause pain and injury to sensitive breast tissue.
– Radiation is cumulative and can induce DNA damage and cancer.
– Extreme psychological distress results from all of the above.
Women are seeking breast imaging options such as automated whole breast ultrasound (ABUS) and QT Imaging.
Women who understand benefits and risks of breast cancer screening are happy to sign a waiver to OPT OUT of mammography.
Insurance coverage for safer options such as ABUS and QT Imaging as stand-alone options are needed.
Having a mammogram — or not — should be a personal decision based on balanced, unbiased information which weighs both the benefits and harms. No one should ever feel pressured, intimidated, bullied, coerced, or shamed for choosing NOT to have a mammogram.
Studies, videos and infographics explaining the scientific facts to support this petition can be found at Be W I S E
Please click the link and consider signing the petition!
INFORMED CHOICE in Breast Cancer Screening / Insurance for Ultrasound and QT Imaging
Please see my pages and posts below focused on PREVENTION & INFORMED CHOICE for EARLY DETECTION:
Women are often told lumpectomy is an easy surgery. One and done.
Yet… more often than not, this is NOT the case. In fact, studies report up to 70% of the time, a 2nd surgery is needed due to “positive margins” for DCIS.
It happened to me in 2011.
After a DCIS diagnosis in January 2010, I chose “active surveillance” plus holistic health strategies.

Fast forward to a “surveillance” mammogram in June 2011 — the alarm bells from doctors went crazy. Calcifications appeared to be growing along with a new area reported as “indefinite” calcifications.
Highly suspicious for malignancy, stated the report. Recommend biopsy of two areas.
I decided to put everything off and go ahead with our summer vacation plans visiting family in Martha’s Vineyard and Denmark. For five weeks, I spent a good amount of my vacation time digging into the research. I also consulted with a Naturopathic Dr. over the phone. She recommended an MRI and also she preferred an “open surgery vs a core needle biopsy” given my situation (known DCIS and now concern of possible invasive cancer.) A needle biopsy posed the risk of missing an area as happened in my case 2 years prior.
Suspicious for malignancy, the MRI report stated.
Deflated, I could feel the fear creeping in. For nearly 2 years, I was diligent with a strict whole food plant based mostly organic diet, and I never missed a day of exercise. My mind now kept thinking about my best friend Dana from college who recently died from cervical cancer. Her two young children were around the same age as mine.
Adding to the stress, my husband was about to change jobs (and insurance).
I decided to take my naturopathic Drs advice: skip the needle biopsy and schedule surgery to remove only the “highly suspicious area.”
Result: NO INVASIVE CANCER, but…
Two positive margins of DCIS.
“A 2nd surgery (re-excision) was needed,” the nurse told me.
Ugh.
I really wanted to be done with it.
Two weeks later, I succumbed to a re-excision.
Result: A “close margin” remains.
This is when my surgeon said to me:
“Your breast is like spoiled soup. It’s not worth saving.”
{WTF!!!}
I got several more opinions and mastectomy kept coming up.
My mind could not wrap my head around this… as DCIS was a “risk factor” — not “cancer!”
Thankfully, I dug further into the research and followed my gut.
I said “NO MORE!”
It’s now over 14 years and I have never had “cancer” — or any other breast issue. (See link to my updated story at end of this post.)
With everything I learned I began to feel angry at “the system” which leads to a never-ending rabbit hole of overdiagnosis and overtreatment — all due to mammography screening.
I would have made different decisions about starting mammography screening at age 40 had I been better informed.
I learned my situation having multiple surgeries for DCIS and then recommendation for mastectomy was not a rare case. Yet this enormous problem is often not disclosed upfront when women are frightened about “cancer” and highly encouraged to have immediate surgery due to calcifications and “abnormal cells” appearing on a mammogram.
“the risk of reoperation in patients with DCIS was 3 times higher than in those with IBC. The widespread use of mammographic screening will increase the number of patients diagnosed with DCIS…”
“This inconsistent definition of a negative margin among clinicians has led to wide variations in the rates of re-excision after lumpectomy. In a study of 54 surgeons, the re-excision rates ranged from 0%-70%.6 Moreover, approximately half of these re-excisions were performed in patients with negative margins (no ink on tumor), with the apparent belief that a wider negative margin would further decrease the rate of local recurrence. Reducing the re-excision rate is an important clinical goal, because re-excisions have the potential to increase patient anxiety, increase morbidity, adversely affect cosmesis, result in patients opting for mastectomy, and increase costs to the health care system.”
“Re-operation rates for ductal carcinoma in-situ (DCIS) have consistently been found to be higher than those of invasive disease, raising concern that patients with DCIS may experience worse outcomes compared to IDC patients.1 Reported re-excision rates for DCIS are highly variable, ranging from 14 to 70%,5 creating uncertainty as to the impact this disease has on patients and the healthcare system.
What is clear, is that increased access and adherence to screening mammography programs has resulted in more malignancies being detected, disproportionately with ductal carcinoma in-situ (DCIS).6 Thus, a clearer understanding of this disease and current treatment are required if outcomes are to be optimized.
While patient, pathologic, and surgeon level factors have been explored in their association with re-excision for invasive ductal carcinoma (IDC),2 fewer studies have been conducted to elucidate these factors for DCIS.”
“All patients with BCS between 1995 and 2017 were included. Patient’s characteristics, pathologic results, and treatments were analyzed. Reoperation rate, type of reoperation, second reoperation, and associated factors of reoperation, mastectomy, and third intervention were determined.
Results: We analyzed 10,761 patients: 1,161 with ductal carcinoma in situ (DCIS) and 9,600 with invasive BC. The reoperation rate was 41.4% for DCIS and 28.0% for invasive BC.”
“Re-excisions are frequent after BCS and are influenced by surgeon volume, patient age, and tumor-related factors. These factors should be considered when counseling patients considering BCS, and also for quality assurance.”
“Anatomic extent of ductal carcinoma in situ (DCIS) may be uncertain in spite of clinical, pathologic, and imaging data. Consequently close/positive margins are common with lumpectomy for DCIS and often lead to a challenge in deciding whether to perform a re-excision or mastectomy.”
The incidence of positive side margins was 20% in BCS and 5% in mastectomies (p < 0.001). Of these patients, 68% and 14% underwent a reoperation (p < 0.001). After a positive side margin in BCS, the reoperation rates according to age groups were 74% (<49), 69% (50-64), 68% (65-79), and 42% (80+) (p = 0.013). Of BCS patients with invasive carcinoma in the side margin, 73% were reoperated on. A reoperation was performed in 70% of patients with a close (≤1 mm) DCIS side margin, compared to 43% with a wider (1.1-2 mm) margin (p = 0.002). The reoperation rates were 55% in invasive carcinoma with close DCIS, 66% in close extensive intraductal component (EIC), and 83% in close pure DCIS (p < 0.001).
“Bilateral mastectomy (BM) increased in frequency from 2004 to 2016 (11–27%). In women < 40 years of age, BM (39%) surpassed [breast-conservation surgery] BCS (35%) in 2010 with a continued upward trend.”
“Despite a steady increase in prophylactic bilateral mastectomies, few women with ductal carcinoma in situ (DCIS) are at risk of developing cancer in the opposite breast, according to the results of a 10-year prospective study presented at the Annual Meeting of the American Society of Breast Surgeons (ASBrS).”
“Doctors have been increasingly concerned that women are choosing bilateral mastectomy in the mistaken belief that it eliminates their future risk of cancer.
Double mastectomies made headlines in 2013, when actress Angelina Jolie had a prophylactic double mastectomy after being diagnosed with a BRCA gene mutation that vastly increases cancer risk.
But 95 percent of breast cancers aren’t caused by BRCA mutations. And most of the women who are choosing double mastectomies haven’t been diagnosed with a BRCA mutation.”
Despite adherence to a 2 mm margin criteria, re-excision rates remain high following BCS for DCIS, with 39% converted to mastectomy when re-excision is required. Intra-operative margin assessment does not appear to reduce re-excisions; in particular, surgeons should be aware of the limitations of specimen mammography for margin assessment in DCIS.
Influence of mammography screening on use of mastectomies in Denmark
Invitations to breast screening and information from public authorities and cancer charities have often promised that screening leads to less invasive surgical therapy [Citation1]. Since the purpose of screening is to find cancer earlier, when it is smaller, it may seem obvious that screening should lead to less invasive surgery. However, screening increases the total amount of surgery because of overdiagnosis of harmless tumours. It also increases mastectomies because of detection of carcinoma in situ, which in the UK constitutes 20% of all screen-detected cancer, and which is treated by mastectomy in 27% of cases compared to 24% of invasive breast cancers [Citation2].
Evidence points to the fact that cancer mortality rates are dropping due to improved treatment, not mammograms.
In February 2009 a group of 24 experts, which included eight professors of epidemiology and public health from around the world, wrote a letter to the Times, drawing attention to the serious harmful consequences of screening associated with the over-diagnosis of breast cancer leading to an increase in the number of mastectomies. Over-diagnosis implies the detection of small non-palpable tumours that, although looking like cancer under the microscope, do not have the potential to develop into life-threatening disease.

I have been contemplating creating this podcast as well as educational videos and a documentary for years.
The intention is to give voice to people who have personal stories of a HEALTH WAKE-UP CALL.
I’m kicking off Episode 1 on this symbolic day with my personal story (see video at bottom of this post).
It was exactly 14 years ago, on January 19th, 2010, I was given a diagnosis that brought my happy life to a screeching halt.
I had never heard of DCIS before, but from the moment I was told about the aggressive treatment protocols, I knew something was not right.
I went home and started to investigate.
I also sent out an email to all my friends and family with the subject line: GOOD NEWS / BAD NEWS.
The good news was DCIS was considered a non-invasive “pre-cancerous” condition and the treatments were to reduce risk of invasive cancer.
The bad news was the aggressive treatments of surgery, radiation and drugs (they were the same as invasive cancer).
My friend Adriana called me and said “No-no-no,” with her Colombian accent. “You mustn’t do these invasive treatments… You must come see me immediately.”

Adriana took me under her wings and began to re-educate me about the human body and its digestive process. She assured me that I had nothing to fear and that our bodies have natural abilities to heal when given the right foods and environment. She taught me about detoxification, building my immune system and alkalizing my body with raw, whole, organic superfoods. Amazingly, as healthy as I thought I was, I had never heard of the alkaline-acid balance and that the foods we ingest become either acid or alkaline in our bodies – and over-acidity can lead to or enhance diseases like cancer. I discovered that many of the foods and beverages I loved were acid-forming, such as: coffee, bread, cheese, jam, cereal, sugar, ice cream, sugar-free gum and beer. I learned that I did not have enough GOOD fat in my diet and I was probably deficient in protein and certain vitamins and minerals because I didn’t eat enough variety of fruits, vegetables, beans and whole grains. Adriana took me to the health food store and showed me how to read ingredients and choose healthier versions of foods. I ate kale and chard for the first time in my life!
Adriana did not go to medical school, but she seemed to know more about cancer than the cancer doctors! She explained cancer to me from a scientific cellular level and assured me that DCIS was NOT cancer and NOTHING to be in fear of. From her perspective, it was the FEAR that was the worst part of a DCIS diagnosis.
Adriana advised me on foods and supplements specific for immunity building and breast cancer prevention. She had me put drops of chlorophyll in my water and gave me a list of foods to eat and to eliminate. She guided me through a two week raw food cleanse including an intensive weekend detox where she whipped up raw soups, tonics and teas round the clock! Adriana told me if I did everything she said and put off doing an MRI for a month, it would be clear. And it was!!!
This changed the course of action I would take for treatment. I was emboldened to say “no” to my team of doctors whose options were a lumpectomy plus 7 weeks of radiation or a mastectomy.

I became fascinated with stories, books, articles and films about holistic ways to reduce cancer risk and improve health. I studied “food as medicine” — and in 2013, I received a Certification in Whole Food, Plant-based Nutrition.
Most importantly what I learned over the last 14 years is this:
True health is more than just high quality organic plant-based food, filtered water and daily exercise. A healthy disease-free life revolves around a mindset. It’s not something most oncologists and healthcare providers are knowledgeable about. One has to go outside of the mainstream medical box and dig deeper within themselves. I made a “Wheel of Healing” that included everything I felt was important to my health and well-being.

I understand how overwhelming it can feel in the beginning after a scary diagnosis. But I also know for sure that this can serve as a wake-up call. It did for me. And while my path is not for everyone, the journey it took me on is one that I am grateful for each and every day.
I created my website DCIS 411 in 2011 in hopes of helping even one person seeking answers and support outside of the mainstream medical box. It warms my heart to know I have made a difference in so many lives. I am truly grateful for the wonderful friendships I have developed along the way.
In 2016, I created a nonprofit called Give Wellness. The mission is simple:

To promote “Wellness as a way-of-life.”
My vision for this podcast is to bring the mission of Give Wellness to a new level. By educating, advocating, supporting and inspiring mind-body-spirit wellness through the power of personal stories.
Thank you for joining me here.
If you’d like to share YOUR HEALTH Wake-Up Call story in an interview format with me, please contact me via email:
dp4peace@yahoo.com
Subject: PODCAST
Your friend in love, light, peace, truth, and health,
Donna Pinto
January 19, 2024
